Short case final practical
General medicine final practical:- short case:
This is an online E log book to discuss our patient's
de-identified health data shared after taking her guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
MUSKAAN GOYAL
Hall ticket no. 1701006120
DEIDENTIFICATION :
The privacy of the patient is being entirely conserved. No identifiers shall be revealed through out the piece of work whatsoever.
CONSENT : An informed consent has been taken from the patient in the presence of the family attenders and other witnesses as well and the document has been conserved securely for future references.
DOA: 7/6/2022
A 22yr old male pt. painter by occupation resident of nalgonda came with
Cheif complaints:
Pain abdomen since 4 days.
HOPI:

Pt. Has started consuming alcohol 4 yrs back due to peer pressure , intially taking one peg per day which has increased to 90ml morning and evening i. e twice daily. He has stopped consuming alcohol 3 months back as advised by the doctor.
Pt. Has history of smoking since 2 yrs . He has been smoking beedies 5 per day till date.
Pt was apparently asymptomatic 3 months back then he developed abdominal pain which was dragging in character for which he was admitted in near by hospital in nalgonda . He was diagnosed with acute pancreatitis and was treated inadequately and was advised to stop consumption of alcohol.
Since then pt has stopped consuming alcohol and has been experiencing alcohol withdrawal symptoms like getting angry , agitation , irritability , craving to consume alcohol, tremors . Pt had consumed alochol 4 days back due to fight with his wife.
In veiw of this symptoms pt.has been brought to psychiatry OPD for deaddiction. He was referred to medicine OPD in veiw of pain abdomen.
Pain was , insidious in onset , started after consuming of alcohol in epigastrium and left hypochondrium which was relieved on bending forward and lying down , aggregated on eating food and standing straight.
No h/o fever , nausea , vomiting.
No h/o chestpain , shortness of breath , constipation
Flatus passed
Past history:
H/o similar complaint in past 3 months back.
No other co morbid conditions
No h/o previous medical surgical history.
Family history :
Not significant
Personal history
Diet : mixed
Appetite : normal
Bowel bladder: regular
Sleep: inadequate
General examination:
Pt was concious coherent and cooperative
Thin built and moderately nourished
Pallor - present
No icterus,cyanosis , clubbing,lymphadenopathy, edema





Nasogastric tube has been placed which is attached to the bag
Vitals at the Time of admission
Temperature- afebrile
Pulse rate- 94bpm
Blood pressure-120/80mmHg
Respiratory rate- 16cpm
Systemic examination:
Abdominal examination:
Inspection:
Shape of the abdomen- flat
Umbilicus is central
No visible scars,pulsations, peristalsis, engorged veins
Palpation:
All the inspectory findings are confirmed.
Tenderness present over the epigastrium and left hypochondrium region
Liver palpable 2cms below costal margin
Liver span: 11.5cm ( normal)
Spleen : not palpable
Kidney : not palpable
Percussion:
No free fluid
Ascultation:
Bowel sounds heard
Other systems:
Respiratory:
b/l air entry present , no added breath sound
CVS :
S1 S2 heard , no added murmurs
CNS :
Higher function intact
No motory and sensory deficit.
Cranial nerves normal .
Investigations:
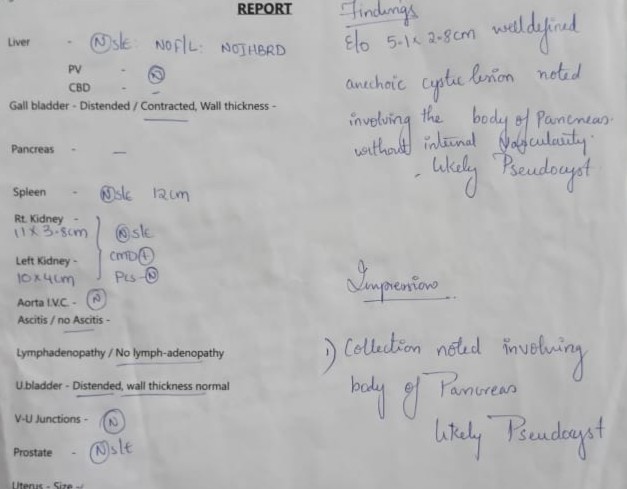
USG abdomen
Serum amylase : increased to more than three times
Serum lipase


Other tests :
Hemogram
RBS
RFT
LFT
Blood grouping




Diagnosis:
Pseudocyst of pancreas secondary to unresolved acute pancreatitis.
Treatment:
Nil per oral
IV fluids Ringer lactate ,Normal saline 100 ml per hour
Inj. Tramadol100mg in 100ml NS IV BD
Inj.pantop 40 mg IV OD
Inj. Optineurin 1 ampoule in 100ml NS IV OD
Psychiatry medication
Tab . Lorazepam 2mg BD
Tab . Benzothiamine100mg OD







Comments
Post a Comment